 I was supposed to be in China today. Since last summer, I’d been planning a trip to China and Taiwan (which was probably also going to include Mongolia), for which I was going to depart this past Saturday. By now I probably would have already walked along the Great Wall, and today I was to fly to Xi’an to see the famed terra cotta warriors. But I’m not in China now; I canceled that trip. Instead of that geographical journey, I’ve embarked on a medical journey. This is the story of an unanticipated medical diagnosis that I received this spring; the life-saving surgery that I’ll need in light of that diagnosis; and how I’m adjusting to what lies ahead.
I was supposed to be in China today. Since last summer, I’d been planning a trip to China and Taiwan (which was probably also going to include Mongolia), for which I was going to depart this past Saturday. By now I probably would have already walked along the Great Wall, and today I was to fly to Xi’an to see the famed terra cotta warriors. But I’m not in China now; I canceled that trip. Instead of that geographical journey, I’ve embarked on a medical journey. This is the story of an unanticipated medical diagnosis that I received this spring; the life-saving surgery that I’ll need in light of that diagnosis; and how I’m adjusting to what lies ahead.
Last month, my world was turned upside down. For the first 45-plus years of my life, I’ve been fortunate enough to have never required an overnight hospital stay — let alone a surgical procedure performed in an operating room. I’ve never been under general anesthesia. Never have I even been hooked up to an intravenous tube. Part of the reason that I’ve been able to travel so frequently during the past few years is that I’ve enjoyed robust health.
But a little more than one month ago, on a Friday afternoon in a cardiologist’s office here in my home city of New York, everything changed. On that Black Friday, I learned that I need to undergo open heart surgery.
What necessitates my surgery is a leaky mitral valve, which can develop from mitral valve prolapse (MVP). The mitral valve, so named because it resembles a mitre (a hat worn by bishops), connects the heart’s left atrium to its left ventricle; MVP occurs when that valve doesn’t close properly. MVP is actually relatively common, and according to the Mayo Clinic, “In most people, mitral valve prolapse isn’t life-threatening and doesn’t require treatment or changes in lifestyle.”
My form of MVP, however, is less benign. In my heart, one of the cords that holds the valve in place has snapped, causing the valve to leak heavily and creating substantial “regurgitation” — i.e., backward flow of blood. This partial reversal of blood flow is forcing my heart to work harder to pump the quantity of blood needed to circulate through my body. Over time, if the problem isn’t addressed, this stress will lead to an enlargement of my heart and a consequent deterioration of its health. In fact, my left atrium has already become slightly embiggened. Ultimately, if left untreated, the leaky valve will result in heart failure. Luckily, the doctors caught my condition early, and a complete fix is available — although they’ll have to open me up in order to make that fix.
The diagnosis that came out of nowhere
Before I talk about my upcoming surgery, you may be wondering how I learned that my heart requires treatment. Often, a cardiac disorder manifests in such symptoms as shortness of breath while climbing stairs, or chest pains. But I’m asymptomatic; my condition hasn’t yet progressed to the stage where such obvious markers of heart disease show up. In my case, it was vigilant doctors who deduced that something was wrong.
As medical diagnostic tools go, it’s difficult to imagine one that’s more low-tech than the venerable stethoscope, invented in 1816. Probably the most clichéd image associated with a doctor’s visit is the M.D. donning the stethoscope to listen to her patient’s heart. So, during a routine physical in March 2015 when my primary care physician placed the stethoscope’s sensor on my chest, I thought nothing of this routine motion that’s played out billions of times in countless examining rooms over the past 199 years. But this time, the end result of my doctor’s listening was far from routine.
After hearing the sound of my heartbeat, my doctor told me that he’d detected something called a heart murmur. (A heart murmur is a whooshing sound caused by abnormal blood flow; in a patient without such a murumur, the only sound audible through the stethoscope is the actual beating of the heart.) Although my doctor assured me that heart murmurs are quite common, he immediately performed an electrocardiogram (EKG) on me in his office. The EKG didn’t reveal any abnormalities.
Nevertheless, my doctor directed me to undergo an additional, non-invasive procedure called an echocardiogram (echo) to “rule out” the possibility of a leaky mitral valve. My doctor didn’t speak with any sense of urgency about the echo, and indeed it took several weeks to obtain the needed authorization from my health insurer and then schedule the procedure. I underwent the echo — a sonogram that bounces sound waves off the heart to generate an image of it — on April 14.
A couple of days later, my doctor called me with the results of the echo. The test had revealed the condition that he’d expected it to rule out: I had MVP and my mitral valve was leaking, causing regurgitation of blood. My doctor added that he would contact the chief of the cardiology department at the hospital where he practices, to set up a consultation with me as soon as possible regarding the echo results. That appointment was set for 8 days later: Friday, April 24.
During the intervening 8 days, I dreaded being told that I would need heart surgery. Some friends and colleagues came forward to tell me that they had MVP themselves — in some cases dating back to their childhoods — and hadn’t required surgical intervention. So I hoped that my case would turn out to be similar to theirs, and that I would prove to be one of the “most people” for whom, according to the Mayo Clinic, MVP doesn’t require treatment. Still, the fact that my primary physician wanted me to meet with not just any cardiologist, but the head of the department, suggested to me that he took my leaky mitral valve quite seriously.
On Friday, April 24, the cardiologist got right to the point. Hopeful of hearing good news, I stated that I understood that many persons with MVP have had it since childhood and haven’t required corrective measures. He responded, “You haven’t had this since childhood.” My mitral valve is leaking “severely,” the cardiologist explained. And I’ll need surgery to repair it within, at most, the next seven years — and, more realistically, within two to three years. Point-blank, he told me that without the surgery I would eventually die. In other words, my heart is a ticking time-bomb.
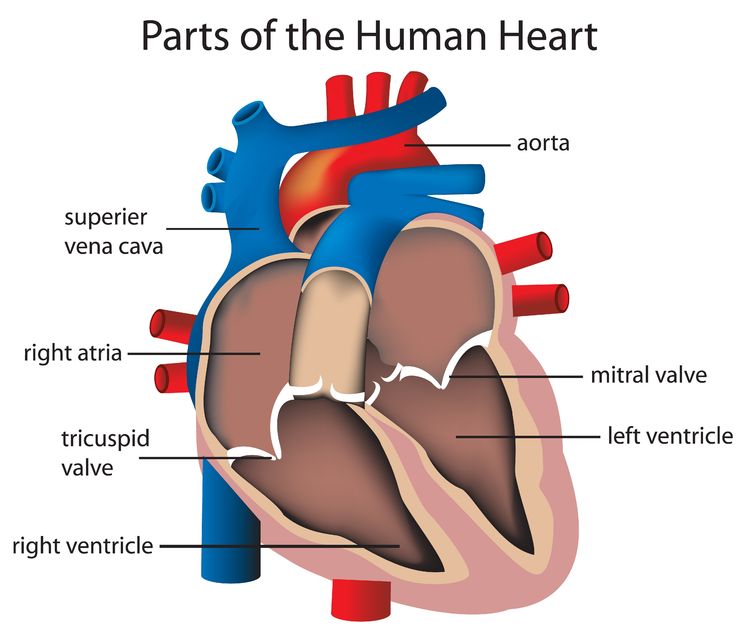
The mitral valve — the part of my heart that has malfunctioned — can be seen on the right of this diagram.
This news stunned me. Prior to receiving my echocardiogram results, I had no known heart problems, nor did any of my immediate family members have a history of heart maladies. I’ve never smoked cigarettes and only drink alcohol in moderation; and I work out regularly at my gym on an eliptical machine for cardiovascular exercise. Thus, heart issues weren’t on my radar. (My cardiologist told me that a predisposition for a mitral valve cord to snap can be genetic in origin, and that the responsible gene can skip a generation. My maternal grandfather died at age 56 after suffering a slew of heart problems that began when he was in his 40s. Although he was a smoker, it seems possible that his cardiac issues could have stemmed, at least in part, from mitral valve leakage that went undetected and thus unaddressed; during his lifetime, echocardiography was in its primitive stages.)
The surgical fix: How can you mend a broken heart?
The needed remedy for my problem is called a “mitral valve repair” and involves the installation of a ring composed of a titanium alloy, to permanently tighten the valve and thereby stop the blood leakage and regurgitation. My cardiologist advised me that the placement of the metallic ring will provide “a lifetime fix.” Another cardiologist whom I subsequently consulted explained that my enlarged atrium will even reduce back to its normal size after the valve has been repaired.
Until relatively recently, in all mitral valve repairs (and in all heart surgeries generally), the surgeons accessed the heart by cracking the patient’s sternum (a/k/a the breastbone). Indeed, the late Robin Williams referred to himself and his fellow alumni of open heart surgery as the “brotherhood of the cracked chest club,” as discussed in this Barbara Walters special. Fracturing the sternum adds an additional element of trauma, the recovery from which sometimes requires several months. It’s fair to say that the brotherhood of the cracked chest club is one fraternity that I have no desire to join.
Within the past decade, however, an important innovation has come down the pike. Valvular repair is increasingly performed via a robotically assisted method: the chief surgeon stands at a high definition video monitor, manipulating endoscopic arms by remote control, and directs those robotic probes as they sew the metallic ring into the patient’s heart to seal the valve. What makes this method such a welcome development isn’t just that it represents cutting-edge technology; it’s that a robotically assisted mitral valve repair it’s significantly less invasive than the way that it’s traditionally been done. In lieu of initiating the patient into the cracked-chest fraternity, the heart is approached via five small incisions in the patient’s side, each about 1 centimeter in length. Those small incisions are all that’s needed to enable the endoscopes to enter the body and penetrate to the heart for the installation of the metallic ring. Thus, the sternum remains unscathed.
The avoidance of smashing through the patient’s sternum is a game-changer, as far as I’m concerned. Having just gotten over a rib contusion for which it took about four months for the pain to permanently subside, I don’t want to endure a similar ordeal with the healing of my sternum. Indeed, I’m informed that due in part to the lack of chest-cracking, and in part to the minuscule size of the incisions, the robotically assisted technique typically results in much less pain for the patient in the aftermath of the procedure; a shorter hospital stay; and a substantially quicker recovery time. What patient wouldn’t want those benefits?
Robotically assisted heart valve surgery is still considered relatively new, although it’s already offered at some of the top hospitals in the United States. Happily, one of the institutions where it’s available is a highly-regarded teaching hospital right here in Manhattan — and the surgeon who performs it there is a global pioneer in robotically assisted cardiac surgery who employed robotic techniques in France as early as 1998. Recently I met with that surgeon, and he informed me that he has about 500 robotically assisted mitral valve repairs under his belt, and that he hasn’t lost a patient during any of those repairs. If I opt for the robotics at his hospital, I’ll be in highly skilled and experienced hands. Well, not literally, because his hands will be manipulating the controls for the robotic arms rather than making direct physical contact with my body. But you know what I mean. 🙂

In just a few months, I’ll be in an operating room like this one. Well, not exactly like this one, because it will probably also include state-of-the-art robotic equipment.
Naturally, I’ve approached my exploration of my treatment options with the same thoroughness and attention to detail with which I plan my travels. 🙂 By sometime in mid to late June, I should be in position to decide which surgical option to select. Obviously, I’m leaning heavily towards going for the robotics. My research does indicate that robotically aided surgery has become increasingly common for a wide variety of types of operations, ranging from hip replacement to gall blader removal, and seems certain to be the wave of the future. In the specific realm of mitral valve repair, the robotically assisted procedure appears to be sufficiently proven and safe that its overwhelming benefits justify its selection.
Incidentally, as you may have guessed from the section heading above, a certain song by the Bee Gees has become an earworm for me during the last few weeks:
In case you’re wondering, I have no plans to attempt this song at karaoke. The falsettos of the Bee Gees are way above my vocal range. 🙂
Confronting my fears
With or without robots, I’ll need to undergo open heart surgery — meaning that the function of pumping my blood, as well as the respiratory function, will be diverted to a heart-lung machine, also known as a cardiopulmonary bypass pump, for the duration of the procedure (which I understand will be approximately one and one-half hours). After the installation of the metallic ring, my heart will be restarted, and I’ll resume breathing through my lungs.
Although the first successful use of a heart-lung machine occurred all the way back in 1953, and open heart surgeries have been performed with high survival rates since the 1960s, I’m still nervous about the fact that my heart will be stopped during the operation. By all accounts, cardiac surgeons have the use of the heart-lung machine down to a science; but dependence on such a machine — which essentially amounts to being on life support — for about 90 minutes is still a fearsome prospect for me. Just the words “open heart surgery” are terrifying to say — although I’m rapidly getting used to uttering those words.
Further sources of nervousness that the surgery presents for me:
• I’ll be knocked out via general anesthesia, which is uncharted territory for me. What if I never wake up after being anesthetized? There’s a non-zero chance that I could die on the operating table. What the doctors refer to as the “mortality risk” of my surgery is low (it’s been quoted to me as 1-2%), but is higher than for many other types of surgeries. I’m not ready to die, but I don’t get to control whether that outcome occurs. (Of course, without the surgery, I would have a 100% chance of eventually perishing from my heart condition.)
• Assuming that I do awaken, the anesthesia involves a particular source of discomfort that I’m not looking forward to. Patients who are given general anesthesia are “intubated” — that is, a tube is inserted down their throat so that they can breathe properly during the surgery. Usually, the tube is removed before the patient awakens. For some reason, in open heart surgery, the patient remains intubated for a period of time after regaining consciousness (although I was told that the surgical team tries to “extubate,” or remove the tube, as quickly as possible). A friend who underwent an open heart procedure a couple of years ago told me that when he woke up and sensed the tube in his throat, he felt like he was choking – and that this sensation felt interminable to him.
• Cardiac surgery also carries a slight risk that that patient will suffer a stroke (although that risk is lower in younger patients).
• My pain tolerance is low. I, who can barely tolerate the insertion of a needle into my arm for bloodwork, am apprehensive about having multiple tubes running into my body for probably two or three days after the operation. (From what I’ve been told, those conduits will include a tube running out of my chest for drainage; a urinary catheter; and of course an IV.)
• I’m a high-maintenance sleeper who always seeks out hotels with blackout drapes in the guestrooms, and requests rooms located away from noisy elevators or ice machines. How will I be able to sleep in a hospital room with the sounds of beeping machines in the background, and with nurses constantly entering the room to check up on me?
The timing of my surgery: I know what I’ll be doing this October
Despite my trepidation, I’m leaning towards having the surgery later this year — most likely in early October. Yes, I probably have a window of a few years in which to deal with it. But the sooner I get the operation over with, the shorter the time that I’ll have the prospect of it hanging over my head, and the sooner I’ll be able to get on with my life. Plus, the younger I am as a heart surgery patient, the lower the risk of complications and the swifter will be my expected recovery. Also, given that the only elective aspect of my surgery is its timing, to put it off significantly past October would just amount to kicking the can down the road.
Naturally, I’ll keep you posted as I schedule, and prepare for, the surgery. Don’t worry, this website isn’t going to turn into a medical blog; I intend to publish plenty of posts about travel and/or karaoke between now and October. 🙂
And somehow I’ll manage to make it through the discomfort that I can expect in the days immediately following the operation. Perhaps the coping mechanism employed by Kimmy Schmidt will help me through those difficult days.
As for my terror of something going wrong during the surgery itself, I’m gradually gaining acceptance of the fact that the risks are something I’m just going to have to deal with. I keep reminding myself that the members of my surgical team will be a group of people who are highly proficient at their jobs, and will do everything in their power to ensure that the operation proceeds smoothly and safely. And I’m trying to train my mind to expect a positive outcome. It helps that my family members, friends, and work colleagues have been amazingly supportive, and have done their best to keep me in good cheer.
Maintaining perspective: Things could have been much worse
I feel fortunate to live in a city in which, regardless of which surgical option I select, my operation will be performed in a world-class hospital by a top-notch team of heart surgeons (technically referred to as cardiothoracic surgeons), anesthesiologists, and other specialists. (Among those additional specialists are the professionals who operate the heart-lung machine; they’re known as perfusion technologists.) I know that I’m also lucky that my job provides me with health insurance that will cover all of the costs of the surgery and hospitalization.
More generally, I’m trying to keep my medical situation in perspective, and to acknowledge additional reasons that I’m lucky despite facing open heart surgery. For example, I recently learned that the wife of a college friend of mine needs a heart transplant — a more complicated and frightening procedure whose long-term prognosis is less sunny. And unlike me, my friend’s wife can’t control the timing of her operation; she has to wait until a “match” (a heart that is adjudged to be a fit for her based on various factors) becomes available. Until that match is found, her own heart will continue to degenerate.
While the heart surgery that’s been prescribed for me will still be no picnic, at least my heart can be healed. Every day, patients — many of whom are much younger than I — are diagnosed with terminal conditions such as late-stage melanoma, or an inoperable brain tumor. I’m lucky in comparison with such patients, many of whom also suffer greatly before the “Big C” finally ends their lives. Even people who win their battle with cancer often achieve that victory only after enduring painful biopsies, and/or treatments such as chemotherapy or radiation therapy that are accompanied by horrible side-effects.
Nor have I been so unfortunate as to be one of those people who, like the husband of Facebook COO Sheryl Sandberg, pass away suddenly and without warning. Earlier this month, even the prosaic act of riding a train between Washington, D.C. and New York City turned deadly for eight passengers who were in the wrong seats at the wrong time.
I’m grateful that in contrast to such other scenarios, mine doesn’t present the specter of sudden or certain death. My medical malady can be remedied, and that’s a great gift.
What all of this means for my travel plans
As stated, in the wake of my diagnosis, I postponed my China trip. My cardiologist has opined that at this point in time, it’s perfectly safe for me to travel, including on airplanes, since I’m still a long way off from developing symptoms from my leaky mitral valve. However, I wasn’t up for being 7,000 miles and 12 time zones away from my support network back here in NYC — not when I’m still processing the fact that my heart will be operated on before the year is out and still going through so much anxiety about that impending procedure. I didn’t need to add jet lag and ultra long-haul airline flights into the mix. So I plan to reschedule my trip to China and its vicinity for the same time next year, by which point I should be long recovered from the surgery (assuming that I have the operation performed in October).
On the other hand, I have two much shorter trips scheduled for prior to October, both of which I intend to go ahead with: a visit to Mount Rushmore, in the State of South Dakota, during America’s Independence Day weekend in early July; and my annual visit to Las Vegas for the Trivia Championships of North America in mid-August.
It goes without saying that after the surgery, I intend to resume my World Karaoke Tour, and international travel generally, as soon as I receive medical clearance to do so. I have a scheduled trip to Rome, which I’ve already had to put off twice, and which is currently slated for late November during America’s Thanksgiving weekend; I hope I’ll be up to finally voyaging to the Eternal City at that time. More doubtful will be my ability to attend the annual travel bloggers’ conference called TBEX (Travel Bloggers’ Exchange) in Fort Lauderdale at the end of October; that just might be too soon after my hospital discharge for me to go out of town.
Life lessons and further thoughts
Throughout my life, I’ve been hospital-phobic. Even visiting other people who’ve been hospitalized has made me uncomfortable and uneasy. Now I’ll be the guy on the operating table and then — assuming all goes well — in the hospital bed. That’s a lot to get used to. I’m trying to draw strength, courage, and inspiration from fellow travel bloggers and other friends who’ve undergone major surgery in the past year, such as Leah of the website Leah Travels — as well as Dave of the website The Planet D, who didn’t have surgery but endured a litany of agonies after fracturing two vertebrae in his back. All have made full recoveries. If they can do it, I can do it!
One takeaway for me from the experiences of people such as Leah and Dave is that the passage of time is a wonderful thing. While the date of my surgery will inexorably arrive, time will continue to flow forward from that point; and before I know it, my surgery, and all of the pain and discomfort associated with it, will be in the rear-view mirror. Of course, the sentiment that “this too shall pass” is hardly a novel one.
Although I haven’t yet gone under the knife, my outlook on life has already changed. The observations that I’ve made about the world around me since the time of my diagnosis — as well as the diagnosis itself — have underscored for me that life is fragile and can turn on a dime. While we’re all fated to shuffle off this mortal coil eventually, you never know when an accident or unexpected medical development might hasten your own demise — or at least subject you to excruciating pain and/or discomfort. You can never take continued good health for granted.
Recognizing these realities has only heightened in my mind the importance of seeing and experiencing as much of the world as possible, for as long as I’m able to do so — to make the most of the opportunities that I’m given. Moreover, no matter where in the world I find myself at any given moment, I’m going to place a greater priority on making every moment count and appreciating every day that I wake up alive.
Earlier in this blog post, I spoke of my friend who felt like he was gagging on the breathing tube when he regained consciousness after his open heart surgery. After relating that memory to me, he asked me if I had any more questions about his experience. “I’m afraid to ask any more questions,” I replied. His response: “I’m alive.” I said, “Yeah, but you went through hell.” His response to that: “Every day is heaven.”

Stock photo of the Mount Rushmore National Monument, which I’ll be visiting in July.



Ow. I’m so sorry to hear this. I am glad to hear, however, that there is a known and reliable procedure.
When you go into the hospital, make sure you (or a friend or relative) bring a box of antiseptic/bleach wipes and wipe down the surfaces in your room. There are far too many cases of staff not doing this, or not doing it properly. You don’t want to have a successful procedure only to get sick because of what the previous patient to share the room had.
Please do keep us posted about any further information as you learn it. We’re all rooting for you and want to see your stories about many more trips on the H-Bomb Karaoke World Tour.
LikeLike
@David C.: Thanks for the support, and for the hygienic suggestion (although the hospital that I’ll probably be having the procedure done at has been rated the safest hospital in NYC for the past two years, and I’m sure they take sanitary procedures very seriously).
LikeLike
I’m really proud of you my ECBFF. I remember talking to you the day after you found out you needed surgery. The state of shock you were you were in mixed with fear. I know those elements still exist, but you are taking all the right steps to handle this mentally and physically. I know I already said it, but I am very proud of you. You have already come this far in the process, and then we will soon be looking back again, saying “look how far you have come”. I hope we can be there – it is our goal. I have learned quite a bit just reading your well written (as usual) post.
LikeLike
@WCBFF: Aww, thanks for the kind words. You know, coming this far in the process has been easy. It’s actually going through the stuff at the hospital that will be hard. I do hope that you and Michael will be able to make it out to New York; your presence there would mean so much.
LikeLike
Thank you for such an open and educational discussion of what you’re going through. I have many of the same fears as I prepare for my upcoming surgery – it’s comforting to know that I am not the only one…
LikeLike
@Erin: Likewise, it’s comforting to know that I’m not the only one experiencing such fears about surgery — although I sure wish that you weren’t going through such an ordeal yourself.
LikeLike